Topical Flucytosine for Yeast Infections
Topical Flucytosine for Yeast Infections
Vulvovagi-what?
Vulvovaginitis, an infection or inflammation of the vulva and vagina, is a common condition that affects women and girls of all ages. Typical presenting symptoms include itching, burning, and abnormal discharge. There are a variety of causes but infections due to bacteria, fungi, viruses, or parasites are the most common etiology. However, sometimes itching and burning can happen without infection and is a result of an allergic reaction or irritation to products such as detergents, fabric softeners, perfumed soaps, spermicides, or vaginal sprays.
Depending on the cause, vulvovaginitis is generally treated with a course of oral or topical antibiotics, antiviral or antifungal drugs, anti-inflammatory agents, or hormonal therapy. However, cases that do not resolve may require maintenance therapy and patients with persistent or unusual symptoms should be referred to a specialist.
Yeast infections
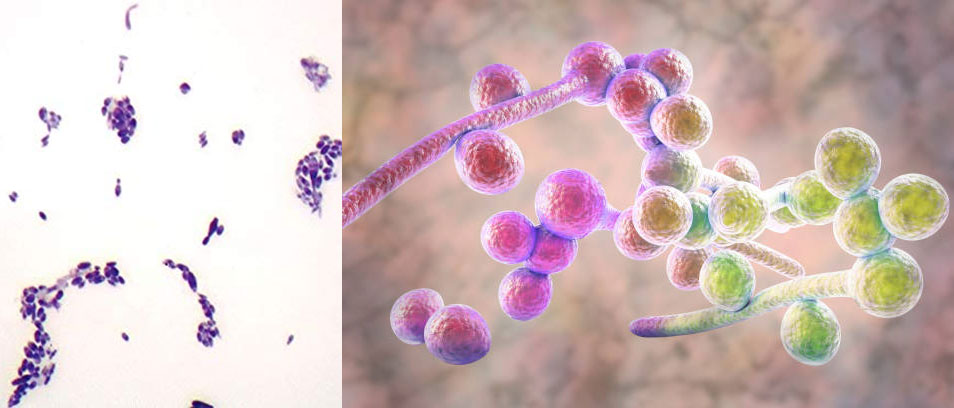
Infections are usually the cause of vulvovaginitis. Common infections include bacterial vaginosis, yeast infections (vaginal candidiasis), trichomoniasis, and herpes simplex virus (HSV). Yeast infections, also called vaginal candidiasis, are caused by fungi and Candida albicans is responsible for most infections. While the vagina naturally contains a balanced mix of yeast and bacteria, this balance can be disrupted, leading to the overgrowth of yeast. This can result from antibiotic use, pregnancy, uncontrolled diabetes, an impaired immune system, and taking oral contraceptives or hormone therapy that increase estrogen levels.
Diagnosis and treatment
Yeast infections can be clinically diagnosed on the basis of cottage cheese-like clumpy discharge, external dysuria (burning sensation while urinating), and vulvar itching, pain, swelling, and redness. Saline microscopy, fungal culture, and DNA tests can also be helpful in the diagnosis.
For mild to moderate symptoms and infrequent episodes, your doctor might recommend:
- Short-course vaginal therapy for 3-7 days. Antifungal medications available as creams, ointments, tablets, and suppositories include miconazole (Monistat 3) and terconazole.
- One-time, single oral dose of fluconazole (Diflucan). To manage more severe symptoms, you might take 2 single doses 3 days apart.
Yeast infections that won’t fully go away
Recurrent candidiasis is defined as 3 or more yeast infections in 12 months. In cases caused by Candida albicans, patients should follow their initial treatment with maintenance therapy (since resistance to antifungal therapy is rare). This is usually done with fluconazole (Diflucan) 150 mg orally for 6 months. Other options include ketoconazole (Nizoral) 100 mg daily and itraconazole (Sporanox) 100 mg daily.
Unfortunately, most of the antifungals used for Candida albicans are not effective against other types of Candida, which are often the culprits of recurrent infections. In other words, since the common antifungals do not work against resistant fungi, the infection will never be fully eradicated. Candida glabrata is particularly common in recurrent episodes and should be treated with one of the following, as they have been used successfully:
- Vaginal boric acid 600 mg daily for 14-21 days
- Flucytosine 15.5% vaginal cream, intravaginally administered as 5 g for 14 days
- Amphotericin B 50 mg vaginal suppositories for 14 days
While boric acid is readily available, flucytosine vaginal cream and amphotericin B vaginal suppositories must be compounded by a pharmacist.
Flucytosine
Flucytosine is an oral antifungal agent that is used with amphotericin B for serious Candida and Cryptococcus infections. It works by penetrating fungal cells and interfering with fungal RNA and protein synthesis. However, it is generally used second-line and its use is limited by its toxicities. Flucytosine should be used with extreme caution in patients with kidney dysfunction and dose adjustments are required. It should also be used with caution in patients with bone marrow depression, hematologic disease, or who have been treated with radiation or drugs that suppress the bone marrow.
Topical flucytosine for yeast infections
Topical flucytosine for the treatment of yeast infections has not been extensively studied. One retrospective study compared the treatment outcome and safety of topical boric acid and flucytosine in women with Candida glabrata yeast infections. Flucytosine cream was offered to 30 patients, 26 of whom had previously received boric acid therapy, with either short-term failure or relapse. Of the 30 patients, 27 patients achieved cure (90%) with flucytosine, while negative cultures were only seen in 64% of patients treated with boric acid. Furthermore, all patients completed and tolerated topical flucytosine therapy and no staining of underclothing and sheets were reported.
There have also been a few case reports reporting successful treatment of refractory vaginal Candida glabrata infections with combined flucytosine and amphotericin B in lubricating jelly. Similarly, the treatment was well-tolerated with no or minimal side effects.
Topical flucytosine is not available commercially but can be compounded at CareFirst Rx Specialty Pharmacy.
References
- https://www.mayoclinic.org/diseases-conditions/yeast-infection/diagnosis-treatment/drc-20379004
- https://www.webmd.com/women/guide/sexual-health-vaginal-infections#2
- Clev Clin J Med. 2017;84(3):215-224.
- Am J Obstet Gynecol. 2003;189:1297-300.
- Am Fam Physician. 2001;63:697-702.
- Sex Transm Inf. 2001;77:212-213.
- Flucytosine in Lexicomp.
Related Products
-
Flucytosine Vaginal Cream Compounded
Flucytosine is an antifungal agent that is used with amphotericin B for serious Candida and Cryptococcus infections. It works by penetrating fungal cells and interfering with fungal RNA and protein synthesis.
Read MoreFlucytosine Vaginal Cream CompoundedAs low as $49.95

Comments