Hair Loss in Men and Women: Diagnosis and Treatment Options
Hair Loss in Men and Women: Diagnosis and Treatment Options
Alopecia commonly referred to as hair loss is a condition that affects the majority of the population. It is more prevalent in males; about 30% of men experience hair loss by the age of 30, 50% by the age of 50 and increases 80% by the age of 70. It is less prevalent in females and about 40-50% of women experience hair loss by the age of 70.
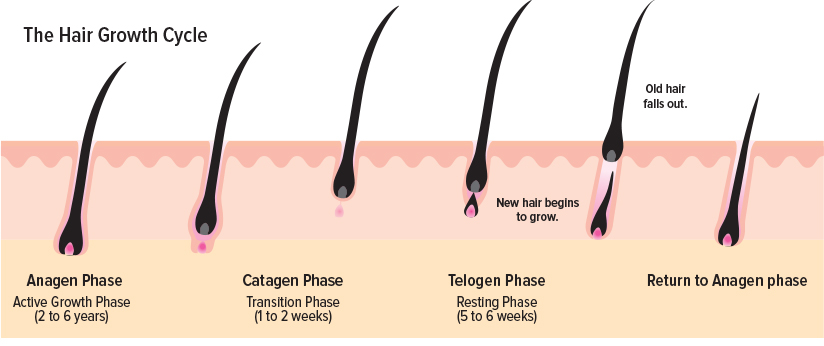
- Anagen (Growth phase): Hair growth is stimulated by the nourishment of hair follicles via blood supply. This phase lasts for 2 to 6 years.
- Catagen (Transition phase): Hair follicles detach from the nourishing blood supply. This phase lasts for 1 to 2 weeks.
- Telogen (Resting phase): The hair dies and falls out without nourishment. This phase lasts for 5 to 6 weeks.
During a normal hair growth cycle, 80-90% follicles are in the growth phase. Around 75 follicles shed hair each day and the same number enter a new growth phase to maintain the balance between growth and loss. This balance can be disrupted due to multiple reasons which ultimately results in hair loss:
- Hormonal changes: Menopause, pregnancy, polycystic ovary syndrome
- Physiologic stress: Surgery, trauma, fever, and infections
- Chronic illnesses: Thyroid disorders, diabetes, lupus, rheumatoid arthritis, anorexia, HIV etc.
- Diet: Rapid weight loss, strict vegetarian diet, protein deficiency etc.
- Local trauma: Tinea capitis (fungal infection of the scalp), compulsive hair pulling
- Genetics: Presence of HLA genes (HLA-DRB1*0401 and DQB1*0301)
Hair loss can be categorized into different types depending on etiology. Identifying the correct hair loss type is important to determine appropriate treatment. The different types of hair loss are:
- Androgenetic alopecia (AGA): Hereditary hair loss with gradual onset. It is the most common type of hair loss and accounts of 95% of all hair losses. It affects both males and females. Males experience loss of the frontal hairline whereas females experience thinning of the central scalp. A variety of commercial and compounded medications are available for treating AGA.
- Alopecia areata: Autoimmune condition with an abrupt onset. It occurs in any hair-bearing area and results in patchy or complete hair loss. It can occur at any age and is due to genetic factors and/or stress. The immune system attacks the hair follicles resulting in hair loss usually in clumps. The most common treatment options include corticosteroids (injections into the scalp, topical and oral formulations) and topical immunotherapy.
- Anagen effluvium: Hair loss that occurs during the growth phase of the hair growth cycle and results in rapid shedding of hair. It is usually a side effect of chemotherapy and radiation. It is a reversible condition and hair grows back 1-3 months after discontinuing the offending agent.
- Telogen effluvium: Hair loss that occurs during the resting of the hair growth cycle and results in rapid shedding of the hair. It usually occurs due to metabolic/hormonal disturbances. Treating the underlying condition can reverse the condition and promote regrowth of hair.
- Cosmetic hair damage: Hair loss that occurs due to broken/damaged hair. It occurs due to tight braiding, constant bleaching and hair treatment with chemicals.
- Trichotillomania: Psychiatric illness characterized by pulling out hair from the scalp, eyebrows and other areas of the body. It is a mental disorder and the patient should be appropriately referred to and managed by a psychiatrist.
- Tinea capitis: Superficial fungal infection of the scalp which results in hair loss. It is contagious and very common in children. Mild cases are treated with topical antifungals. Oral antifungals and a short course of steroids can be added to therapy for severe and/or resistant infections.
Androgenetic alopecia:
It is the most common type of hair loss and the difference in pattern between males and females is demonstrated below.
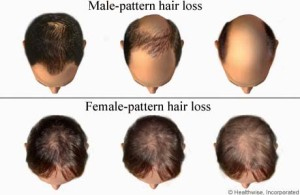
- Male-pattern hair loss: Loss of the frontal hairline.
- Female-pattern baldness: Thinning of the central scalp.
The exact mechanism of hair loss in not known, however, there is a relation between the levels of dihydrotestosterone (DHT) and hair loss, especially in males.

DHT results in the shortening of the growth phase resulting in smaller hair follicles. This process is known as miniaturizing hair. Over a period of time, the hair follicles get smaller and smaller which ultimately result in very few visible hair.
Due to the identified role of DHT in hair loss, a lot of the treatment options target DHT to promote hair growth. AGA is diagnosed by examining the scalp and ordering blood tests to identify underlying causes such as abnormal hormonal levels, iron deficiency anemia and thyroid problems.
Treatment options:
-
Minoxidil: It increases blood flow to the hair follicles and prolongs the anagen (growth) phase to promote hair growth. It is FDA approved for treating androgenetic alopecia and is commercially available as Rogaine in a 2% solution and 2 and 5% foam formulation. Within 2 months the hair begins to shed less and in 4 to 8 months new hair should begin to grow. Its effectiveness is dose dependent and higher strength formulations cause more hair growth. Results are seen as early as 2 months. High strength formulations are not available commercially as it is not soluble in the standard liquid base. However, it can be compounded at a specialty pharmacy in a cream or lotion base once prescribed by the provider. Commercially available products are only effective in 30-40% people. Majority of the population will require high strength minoxidil or combination products to experience optimal results.
Directions: Apply to a clean and dry scalp and allow 2-4 hours for the drug to penetrate the scalp. The scalp should be free of cuts or opening, applying over here can result in the absorption of the drug into the bloodstream. The effectiveness of minoxidil stabilizes after 12 to 18 month of use. It has to be continued indefinitely as discontinuation results in the loss of newly grown hair.
Side effects: Itching, irritation, dryness, and hypertrichosis. Avoid in pregnancy and patients less than 18 years of age.
-
Finasteride/Dutasteride: They are 5-The image inhibitor and prevent testosterone from breaking down into DHT, which is the hormone responsible for male pattern baldness. They are commonly used to treat Benign prostatic hyperplasia (BPH) and urinary incontinence in males at higher doses. Finasteride is FDA approved for treating hair loss at a lower dose and is commercially available under the brand name Propecia. It works synergistically with other ingredients to promote hair growth and can be compounded topically in combination with minoxidil and other drugs discussed below. Avoid using oral and topical finasteride together as it can increase the risk of side effects. It is not effective in most women and may require alternate agents.
Side effects: Weakness and dizziness are commonly seen. With higher doses, patients can experience erectile dysfunction and decreased sex drive. It is not safe to use in pregnant women, including touching the pill.
-
Spironolactone: It decreases the production of hormones such as androgens which are responsible for causing AGA. It is used as add on agent for female-pattern baldness when minoxidil is ineffective. It can be administered orally or in combination with other products such as minoxidil topically.
Side effects: Dizziness, sleepiness, breast tenderness, and elevated potassium levels. It is not safe to use in pregnant women.
-
Latanoprost: It acts as a prostaglandin which is a naturally occurring substance in the body which plays a role in hair growth. It is FDA approved for treating glaucoma and eyelash alopecia. Studies show that if applied topically to the scalp it can stimulate hair growth and significantly increase hair density. Effects are seen as early as 24 weeks of treatment. It is often compounded in combination with minoxidil.
-
Corticosteroids: It is a steroid hormone which decreases the inflammation and suppresses the immune system. It is often used in conjunction with minoxidil to decrease the inflammation and irritation with higher strengths. It is commonly used to treat in alopecia areata as injected, topical, oral or any combination of the three formulations.
Side effects: Topical formulation redness and thinning of the skin. Oral formulations are associated with weight gain, high blood sugars, swelling of legs, glaucoma etc.
-
Progesterone: It is a hormone produced by both men and women which competes with 5-alpha reductase and prevents the conversion of testosterone to DHT. As you get older, progesterone decreases causing increased production of DHT which results in hair loss. Progesterone can be administered orally or topically compounded to stimulate hair growth.
Side effects: Acne, insomnia, breast tenderness, fluid retention, headaches, depression. These are commonly seen with oral or high doses. The lower dose and topical formulations are generally well tolerated.
-
Estrogen: Estrogen is directly associated with hair growth. Higher levels of estrogen are associated with thicker, fuller hair. Low estrogen levels during menopause or after pregnancy cause hair to enter the resting phase resulting in hair loss. Estrogen supplementation is a good treatment option for women suffering from AGA due to low estrogen levels. Depending on the severity and presence of other conditions it can be prescribed as an oral or topical agent. Along with hair loss, it can also help with post-menopausal symptoms such as hot flashes, difficulty sleeping, and decreased sex drive.
Side effects: Slightly increased risk of breast cancer, increased risk of blood clots, heart disease, and stroke. These side effects are seen with higher oral doses. The lower doses and topical formulations are generally well tolerated.
-
Azelaic acid: It is a scavenger of oxy radicals and inhibits 5-alpha reductase preventing the conversion of testosterone to DHT. It decreases the free fatty acid content of the skin surface lipids to help maximize the absorption of minoxidil. Hence, it can be used alone or in combination with minoxidil topically.
Side effects: Burning, itching, tingling, redness, irritation of the skin.
-
Tretinoin (Retinoic acid): It improves the absorption of minoxidil into the scalp by acting as a skin peel and increasing the permeation of minoxidil to the lower layers of the skin where hair follicles are located. It also promotes vascular proliferation which is important for hair regrowth. It is compounded in combination with minoxidil topically to increase hair growth by up to 100%.
Side effects: Burning, stinging, irritation, peeling and crusting of the skin.
-
Transplant: Surgical treatment option for hair loss. The healthy follicles from other parts of the scalp are transplanted to the bald area. It is considered a cosmetic procedure and is mostly not covered by the insurance and can be very expensive.
Side effects: Bleeding, infection, swelling of the scalp.
-
Platelet-rich plasma (PRP): It increases the blood supply to the hair follicle and triggers hair growth. It consists of three treatments in 4-6 week periods followed by maintenance treatment every 4-6 months. It is divided into three steps:
- Patient’s blood is drawn and put in the centrifuge for 10 minutes
- Blood separates into three layers platelet-poor plasma, platelet-rich plasma, and red blood cells
- Platelet-rich plasma is then injected into the scalp
Side effects: Injury to blood vessels or nerves while injecting, infection, calcification and scar tissue at the injection site.
-
Cetirizine: It is a second generation anti-histamine and also inhibits prostaglandin D2 which has some role in hair loss. Some studies have shown that using 1% topical cetirizine showed significant improvement in hair growth. The anti-inflammatory properties of cetirizine can also help with scalp inflammation and irritations.
-
Biotin: It is a vitamin which has proven benefits for hair growth and is only effective if the patient is biotin deficient. It has no role on the DHT levels. It can be ingested orally or compounded topically to facilitate hair growth.
A variety of topical products can be compounded to meet your needs. Some examples are:
- Minoxidil (high strength)
- Minoxidil/Finasteride topical solution
- Minoxidil/Finasteride/Azelaic acid/Progesterone/Tretinoin topical solution
- Fluocinonide/Azelaic acid/Minoxidil/Tretinoin shampoo
- Latanoprost/Finasteride topical foam
- Minoxidil/Finasteride/Spironolactone topical foam
- And many more!!!
References
- Types of Hair Loss. Can be accessed at https://nyulangone.org/conditions/hair-loss/types. Retrieved on February 20, 2019
- Olsen EA. Androgenetic alopecia. In: Disorders of hair growth: Diagnosis and treatment, Olsen EA (Ed), McGraw-Hill, New York 1994. p.257.
- Camacho-Martínez FM. Hair loss in women. Semin Cutan Med Surg 2009; 28:19.
- Kaufman KD, Olsen EA, Whiting D, et al. Finasteride in the treatment of men with androgenetic alopecia. Finasteride Male Pattern Hair Loss Study Group. J Am Acad Dermatol 1998; 39:578.
- Rossi A, Campo D, Fortuna MC, et al. A preliminary study on topical cetirizine in the therapeutic management of androgenetic alopecia. J Dermatolog Treat. 2018;29(2):149-151.
- Lexi-Drugs. Lexicomp. Wolters Kluwer Health, Inc. Riverwoods, IL. Available at: http://online.lexi.com. Accessed February 20, 2019.
- Figure 1: Hair growth cycle. The image can be accessed at https://www.toppik.com/hairtoppiksblog/understanding-hair-growth-cycle/anatomical-training-poster-hair-growth-phase-step-by-step-stages-of-the-hair-growth-cycle-anagen-telogen-catagen-skin-anatomy-cross-section-of-the-skin-layers-medical-vector-illustration/ Retrieved on February 20, 2019.
- Figure 2: Male and female-pattern hair loss. The image can be accessed at http://www.pcds.org.uk/clinical-guidance/alopecia-male-and-female-pattern-alopecia Retrieved on 2/20/19. Retrieved on February 20, 2019.
- Figure 3: DHT and hair loss. The image can be accessed at https://www.womenscenterforhairloss.com/hair-loss-in-women/hereditary-hairloss. Retrieved on February 20, 2019.
Related Products
-

Minoxidil / Finasteride / Tretinoin Topical Foam / Solution Compounded
Our Minoxidil Topical can be compounded with other ingredients
Read More -

Tretinoin Topical Compounded
Tretinoin is a medication used to treat acne vulgaris. It promotes the exfoliation of affected skin areas and unclogs pores. Tretinoin controls skin break out yet does not cure it.
Read MoreTretinoin Topical CompoundedAs low as $54.95 -

Clindamycin / Tretinoin Topical Gel Compounded
Clindamycin inhibits bacterial protein synthesis at the level of the bacterial ribosome.
Read MoreClindamycin / Tretinoin Topical Gel CompoundedAs low as $54.95 -

Imiquimod / Tretinoin Cream Compounded
Read MoreImiquimod / Tretinoin Cream CompoundedAs low as $54.95 -

Minoxidil / Clobetasol / Tretinoin Solution Compounded
Our Minoxidil Topical can be compounded with other ingredients
Read MoreMinoxidil / Clobetasol / Tretinoin Solution CompoundedAs low as $69.95 -

Hydroquinone/Tretinoin Cream Compounded
Hydroquinone is used for hyperpigmentation, melasma, dark spots and freckles.
Read MoreHydroquinone/Tretinoin Cream CompoundedAs low as $74.95 -
Metformin HCL/Progesterone/Azelaic Acid Cream Compounded
Metformin is an anti-diabetic medication and is generally the preferred initial pharmacologic agent for the treatment of diabetes mellitus 2. It is also used for antipsychotic-induced weight gain, polycystic ovary syndrome (PCOS), gestational diabetes mellitus, and other conditions. Here at CareFirst Specialty Pharmacy, we have the facility capable of compounding metformin into different dosage forms such as creams and capsules to best fit your needs.
Read MoreMetformin HCL/Progesterone/Azelaic Acid Cream CompoundedAs low as $79.95 -

Minoxidil / Finasteride / Progesterone Topical Foam / Solution Compounded
Our Minoxidil Topical can be compounded with other ingredients
Read More -

Latanoprost Topical Foam / Solution Compounded
Latanoprost mimics naturally occurring prostaglandin chemicals in the body. Our Latanoprost Topical can be compounded with other ingredients.
Read MoreLatanoprost Topical Foam / Solution CompoundedAs low as $69.95 -

Latanoprost / Finasteride Topical Foam / Solution Compounded
Our Latanoprost Topical can be compounded with other ingredients
Read MoreLatanoprost / Finasteride Topical Foam / Solution CompoundedAs low as $79.95 -

Latanoprost / Minoxidil Topical Form / Solution Compounded
Our Latanoprost Topical can be compounded with other ingredients
Read MoreLatanoprost / Minoxidil Topical Form / Solution CompoundedAs low as $79.95 -

Latanoprost / Minoxidil / Finasteride Topical Foam / Solution Compounded
Our Latanoprost Topical can be compounded with other ingredients
Read More

Comments